
Feline upper respiratory infection
Article written and translated by Coline Borel, unauthorized copying without permission of the author
Definition:
Respiratory pathology is one of the most important subjects of feline medicine. Upper respiratory infection (URI) is a syndrome characterized by inflammatory lesions of the respiratory tract, the oral cavity and the eye. All cats can get sick, but multiple-cat households are more affected because the disease is very contagious.
Etiology:
Various microorganisms are responsible alone or together of the disorder. In order of importance:
- Feline calicivirus (FCV): it multiplies in digestive and respiratory epithelial cells. It is stable in the
environment (8-10 days). As only agent, it causes minor form, characterized by serous nasal discharge and stomatitis. The cat continuously excrete virus for 24 to 30 month in 40% of the cases
without symptoms. Feline calicivirus exhibits a large genetic diversity. Some virus strains are highly pathogen and induce epidemic hemorrhagic fever with death in 40% of the cases (the affected
cats are kittens. They have fever, icterus, respiratory distress and pneumonia, pancreatitis, bad condition.). Two cases have been described in Germany in 2011 (Schulz BS, Hartmann K, Unterer S,
Eichhorn W, Majzoub M, Homeier-Bachmann T, Truyen U, Ellenberger C, Huebner J. Two outbreaks of virulent systemic feline calicivirus infection in cats in Germany. Berl Munch Tierarztl Wochenschr.
2011 May-Jun;124(5-6):186-93.)
- Feline herpesvirus 1 (FVH1): specific virus of the cat, it causes rhinotracheitis by necrosis of the respiratory tract
epithelial cells (the virus multiplies in these cells). The ocular conjunctiva, the cornea and the genital tract can be also affected (corneal ulceration, abortion and neonatal death). The
recovery is slow; the disease is more severe than that caused by FCV. After resolution of the clinical signs, animals become chronic carrier with intermittent excretion because of a latency
phenomenon. The virus is unstable in the environment and only resists for 24 hours.
- Chlamydophila felis: this bacterium is exclusively intracellular and causes ocular conjunctiva and nasal mucosa infection. Excretion lasts 3 to 8
months. It resists few time in the environment.
- Bordetella bronchiseptica: this bacterium is not specific of the cat. It is also responsible of the canine infectious tracheobronchitis. However,
it is specific of the respiratory tract. Its survey in the environment is not known, but it is supposed to be about 10 days. Stress can reactive a primary underlying infection (ex : after a
birth).
- Reovirus: it causes a common URI. This virus is very resistant in the environment.
Epidemiology:
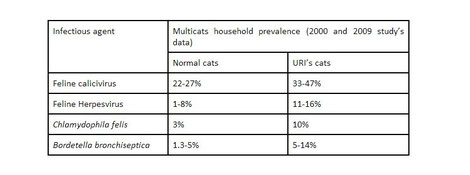
80 to 90% of URI are secondary to FHV1 and/or FCV infection. Until 40% of the multiple cat households are FCV carrier.
Infectious agent's sources are not only clinically affected cats but also asymptomatic cats that are chronic carriers, incubating infection or having recently recovered. In that way, prevention
is difficult to lead.
Virulent materials are secretions (ocular, nasal.) and in a lesser way, feces. The transmission is direct with nose to nose closed contact (especially for the FHV1 because it's unstable in the
environment) or indirect with (mess tin, humans.). Infectious agents use the oronasal and ocular way to enter the organism.
Kittens (of 4-8 weeks) and young cats are the more vulnerable to the disease.
Clinical features:
Clinical signs vary, depending on the agent, the dose and the virulence strain, the age and the physiologic state of the cat.
Incubation is short (2-4 days) and there are 2 forms of the disease:
- Acute form, the most common: fever, sneezing mandibular lymph node hyperplasia, nasal, conjunctival and tonsillar inflammation, serous or mucopurulent nasal and ocular discharge, dyspnea,
cough, oral ulceration, hypersalivation, anorexia and dehydratation. FHV1 can also cause corneal ulceration. The recovery is made in approximately 10 days.
- Chronic form: it's secondary to bacterial complications of the acute form. It can be characterized by sinusitis (in particular on Persians, with sometimes irreversible damages to turbinates and
mucosa by FHV1), pneumonia, ulcerative keratitis, stomatitis, abortion, rare neurological signs or urinary disorders. Underlying causes must be researched (FIV co-infection for example).
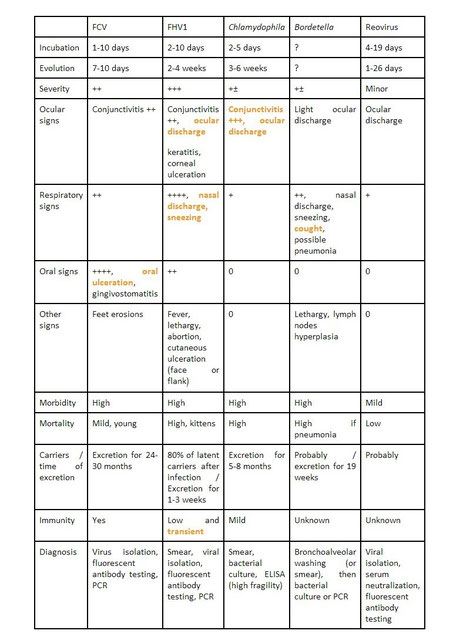
Some clinical signs are more frequently observed depending on the infectious agent. It can help to the diagnosis (very suggestive signs are in red). But be careful, the only way to determine which is/are the incriminated infectious agent(s) is to do laboratory analysis.
Diagnosis:
URI's diagnosis is easy to do with the clinical signs (rhinitis, stomatitis, keratitis, conjunctivitis).
On the other hand, as explained before, it is impossible to determine what are the incriminated infectious agent(s) on the basis of the only clinical signs. This etiologic
diagnosis is essential for the multiple cat households in order to cure and control the disease. PCR (Polymerase Chain Reaction), fluorescent antibody, serum neutralization or ELISA analysis are
performed on pharyngeal, conjunctival and nasal swab. Blood serology is possible but is not interesting for the diagnosis because of false-negative or false-positive results (vaccine
interference, lack of antibody production on acute cases).
Treatment:
For an individual cat, the aim is to eliminate the cause of the URI, to prevent potential complications and residua and to give a supportive care. Even if in most cases, URI is self-limiting, symptomatic and specific treatments are necessary:
- Hydration and nutritional care especially on kittens;
- Anti-inflammatory drugs for the respiratory tract inflammation;
- Antiviral drugs generally or topically with humane eye lotions for corneal ulcers (idoxuridine, trifluridine, ganciclovir);
N.B. : a pilot study in 2012 showed that oral administration of famciclovir (antiviral drug) 3 times per day to cats resulted in a sufficient tear antiviral concentration at the ocular surface likely to be effective against FHV1 (Thomasy SM, Covert JC, Stanley SD, Maggs DJ. Pharmacokinetics of famciclovir and penciclovir in tears following oral administration of famciclovir to cats: a pilot study. Vet Ophtalmol, 2012 Feb 16 doi: 10.1111/j.1463-5224.2011.00984.x.).
- Feline recombinant interferon omega (VIRBAGEN Omega®) by local or general administration with satisfactory results on virus (expensive treatment) (according to results of study in 2007 and
2011);
- Antibiotics (tetracycline, ampicillin, cephalosporin or gentamicine) to prevent and cure bacterial complications and surinfections. They are also used for Chlamydiosis (ophthalmic ointment and
general administration of tetracycline for one month; repeat 6 months later in multiple cat households to avoid recurrence).
- Aerosoltherapy (using dexamethasone, gentamicine, essential oil (+/- acetylcysteine, questioned)) in order to relieve respiratory tract congestion and to locally treat the rhinitis.
In multiple cat households, URI's management is a real challenge for both veterinarians and breeders. The aims are different than a single pet cat: they are to limit the duration of clinical signs and to limit the recurrence. In that way, etiologic diagnosis is essential.
Prognosis:
The prognosis for cats with acute URI is good. Chronic disease doesn't develop on most cats, and nearly all of those with chronic disease have a good quality of life with appropriate supportive care.
Prevention:
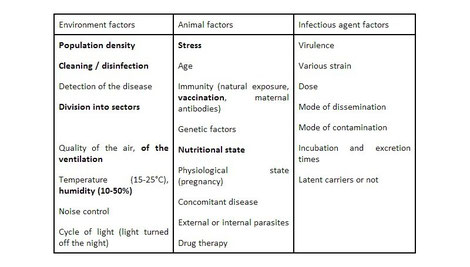
Sanitary prevention is difficult to lead because of the healthy carriers which are source of FHV1, calicivirus and Chlamydophila. They sustain the circulation of these agents in a multiple cat household. The prevention program is based on 3 data : environment, host and infectious agent. So the breeder and the veterinarian should avoid the distribution of the disease in the cattery, should help the immune response of the animal and should control the responsive infectious agent according to its life cycle.
In a general way, the risk of infection should be avoided if the following precautions are taken:
- To isolate affected cats in quarantine. If the space is enough wide, affected cats should be placed in lots (mild affected or clinically cured and severely affected);
- To attend to the general hygiene : to wash hands, to change clothes. Note that, in contrasts to its effect on bacteria, alcohol-based hand gel don't perfectly inactivate the URI's virus
(especially FCV). Bleaching agents that are used in washing machines would have a virucidal effect (Japanese study on FCV in 2012) (Tobe S, Hoshi M, Iizuka K, Tadenuma H, Takaoka H, Komoriya
T, Kohno H. Virucidal effects of bleach activators, sodium alkyl acyloxybenzene sulfonate and acyloxybenzoic acid, against Feline calicivirus. J Oleo Sci. 2012;61(4):211-6);
- To take care of the animals in good health then the more fragile ones (i.e. kittens), then of the adults, and finally of the sick ones. He must walk in only one direction;
- To disinfect the environment. Product will be chosen depending on the infectious agent(s). Several products can be used together: quaternary ammonium is inactive on FCV, bleach 1/30th for 10-15
minutes is active but only after cleaning (organic matter inactivates bleach), potassium peroxymonosulfate (Virkon®), or chlorhexidine (expensive and without effect on FCV). Numerous studies
about virus inactivation (especially on FCV because it's the more resistant) have been performed in the last years with various products and techniques (hydrogen peroxide, chlorine, sodium
chloride, sodium nitrate, heat, ultrasounds, electron beam irradiation.);
- To introduce new cats only after a 3 weeks period of quarantine, including tests and vaccination;
- To isolate pregnant females 3 weeks before birth (in order to limit excretion secondary to the stress) and to avoid contact between young kittens and chronic carriers;
- To early wean kittens if the female is chronic carrier;
-To limit all the stress factors responsible for a decrease of the immunity and for a reexcretion of the agents by chronic carriers. For it, the breeder must decrease the density of cats,
multiply the number of different types of litter box and increase the number of feeding places (organization of the territory), and enrich the environment with games;
- To identify the chronic carriers and the chronic affected cats;
- To supplement FHV affected cats with L-lysine (400 mg q24h orally) in order to limit reactivation and reexcretion of the virus (but complementary studies are necessary to recommend this
treatment for breeding catteries);
- To follow a well-reasoned vaccination program to limit amplification phenomenon.
Most of the vaccines are against feline herpesvirus and feline calicivirus. Some are also against Chlamydophila. Feline calicivirus vaccines insure protection against the majority of
strains but not all. So the effectiveness of vaccination is not the same according to the incriminated agent and strain. But any vaccinated cat which would contract an URI will always
have less severe clinical signs than one which is not vaccinated.
The vaccination program is different depending on the veterinarian vaccines one single cat or a multiple-cat household, because in some breeding catteries, URI is endemic.
Breeding vaccination program:
Whatever the breeding, FHV1 and FCV vaccines are recommended. Regarding Chlamidophila vaccine, it must be used only in the breeding catteries where analysis showed an important circulation of the
agent. Currently, no Bordetella bronchiseptica vaccine exists in France with a marketing authorization for cats (but intranasal Bordetella vaccine exists in other
countries).
All adult cats must be regularly vaccinated (French laboratory recommendations are once a year).
Queens that are not updated for vaccination or that presented clinical signs of URI can have one shot before reproduction period in order to increase the antibodies' level that will be passed on
kittens.
Pregnant and breast-feeding queen mustn't be vaccinated (no safety tests done). Nevertheless, in endemic URI breedings (despite hygiene rules), an inactivated vaccine (killed
vaccine) can be advised on pregnant females.
Vaccination of the kittens depends on the inborn immunity (little developed the first weeks), the maternal antibodies (absorbed in the 24 first hours of live in the colostrum) and the acquired
immunity following upon the vaccination or a natural infection. Maternal antibodies protection is an essential notion because it's frequently the cause of vaccinal failure.
Maternal protection usually disappears around the 9 to 12 weeks of age. But it can disappear earlier (since 6 weeks) if the mum has a poor antibody level or if colostrum intake is insufficient.
In this case, kittens will be effectively vaccinated earlier (some vaccines have marketing authorization on 6 weeks old kittens minimum). On the contrary, maternal protection can disappear later
(at 16 weeks old), so vaccines must be repeated over 16 weeks old to insure a good primary vaccination.
In multiple-cat households, if there are affected kittens offspring of, regularly vaccinated females, the recommended vaccination protocol is to inject 3 shots at 3 weeks of intervals (instead of
2 shots at 8-9 weeks of age and 11-12 weeks of age). For example: shots at 9, 12 and 16 weeks or at 7, 10 and 13 weeks.
A 2012 study shows that 44% of vaccinated kittens have insufficient antibodies levels against FHV1 (4% against FCV) at 17 weeks old. It also shows that antibody protection depends on vaccine
(modified-live or inactivated) and on maternal antibodies (Digangi BA, Levy JK, Griffin B, Reese MJ, Dingman PA, Tucker SJ, Dubovi EJ. Effects of maternally-derived antibodies on serologic
responses to vaccination in kittens. J Feline Med Surg. 2012 Feb;14(2):118-23).
In all cases, vaccination of kittens in breedings must be lead individually with the help and advice of the regular veterinarian.
In conclusion:
Eradication of URI's infectious agents in breedings is difficult because of the chronic, asymptomatic and latent carriers. But rigorous medical and sanitary prevention helps to limit the clinical disease's expression. URI is not inevitability in breeding catteries because, even if it is frequent and almost inevitable in multiple-cat households, it is not a serious illness for young cat promised to an individual pet life.
URI seems inevitable in breeding catteries and is frequent in multiple-cat households. However, it is not a serious illness for young cat promised to an individual pet life.
Sources:
Cadoré J.L., internal medicine lessons of the 3rd year at the National Veterinary School of Lyon, 2006.
Grellet A. Diagnostic et maîtrise du coryza en élevage félin, Le Nouveau Praticien Vétérinaire Canine-Féline, 2010, vol 9 n°44, mai, 50-56.